
Madhukar Pai, McGill University
“Where youth grows pale, and spectre-thin, and dies,” wrote John Keats, in his acclaimed “Ode to a Nightingale.” His words probably summarized his struggle against tuberculosis (TB), an ancient disease that killed millions in his time. Sadly, Keats lost his fight against TB in 1821, and died at the age of 25.
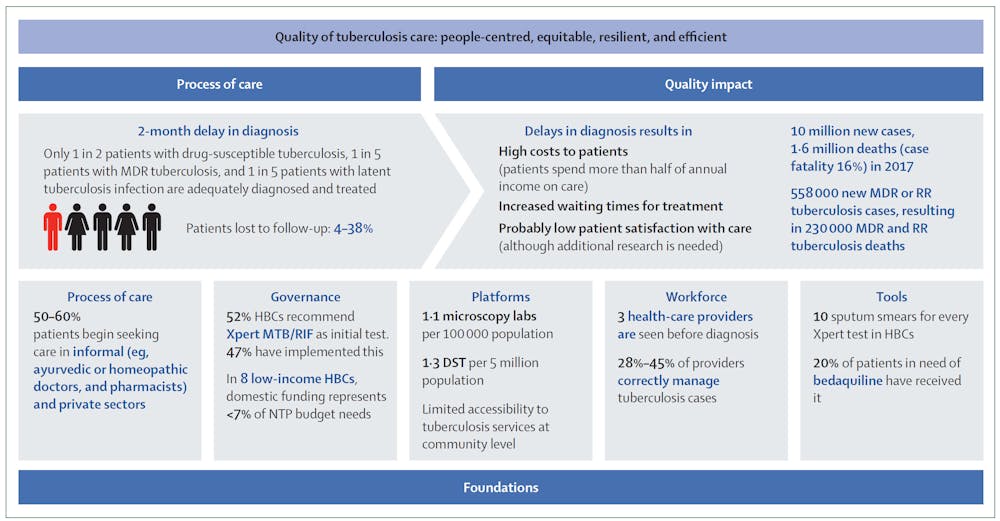
Shockingly, even today, TB kills 1.6 million people a year globally — more people than any other infectious disease. Over 10 million people fall sick with Mycobacterium tuberculosis each year, and nearly a quarter of the world’s population is estimated to be latently infected. The TB epidemic most affects low and middle income countries, with India having the highest burden.
While the world has witnessed dramatic success in tackling infections such as smallpox, polio, malaria and HIV, why are we struggling to imagine and build a world free of TB?
The Lancet Commission on TB, published this week, outlines an ambitious blueprint for ending TB within a generation.
The report, which engaged 37 commissioners from 13 countries, includes economic and modelling analyses and identifies several key priorities. I had the privilege to serve as one of the commissioners.
Quality TB care for all
A key priority is to make sure all persons with TB get quality care, with the best available tools and interventions. Currently, too many persons with TB are getting diagnosed late, struggling to access care and not being supported in navigating the long and expensive treatment process. It is no wonder that half of all TB deaths are attributed to poor-quality care.
Quality care must be available, whether persons with TB seek care in the public or private health sector. The private sector is a major source of health care in many countries and some innovative models for engaging this sector have been proposed — to help reach all patients with TB and also ensure their outcomes are improved.
We simply cannot hope to offer quality care with century-old tools. All countries must modernize their TB-care system, scale-up new rapid molecular diagnostic tests, ensure drug-susceptibility testing for all patients with TB and upgrade treatment guidelines to be consistent with the latest 2019 World Health Organization (WHO) guidelines.
No quality without investments
Massive under-investment is one reason why TB care is so poor in many countries. The Lancet Commission makes a strong case for affected countries, donor nations, the private sector and philanthropists to devise effective financing strategies to end the TB epidemic.
The global cost to reduce TB deaths by 90 per cent (from 1.7 million per year to less than 200,000 a year) could be in the order of US$10 billion a year, and investments would need to increase by about US$5 billion a year.
However, this would be followed by reduced costs (diminishing to US$1 billion to US$2 billion a year by the early 2040s) as there are fewer new cases.
Investing in TB has a strong return on investment, with an estimated US$16 to US$82 return for every dollar spent on TB research and development. Similarly, TB control could produce considerable economic benefits for high-burden countries, with savings three to seven times higher for every TB death averted.
More public finances must be allocated to TB (from increasing GDP levels due to economic development, taxing tobacco and alcohol and by increasing health insurance) in addition to increased investment in health infrastructure.
Countries most affected by TB — especially Brazil, India, China, South Africa and Russia — can and must step up their investments. Donor funding from high-income countries can then be targeted at low-income countries via mechanisms such as the Global Fund.
A human-rights based approach
Currently, TB care delivery systems are designed to suit the health system, not necessarily the person affected by TB.

A good example of this is the requirement for direct observation of TB therapy (DOT), which requires patients to swallow pills in front of health-care workers. A human-centred design approach is necessary to respond to patient needs, including access to peer counselling, mental health care during and after treatment, rehabilitation after therapy and respectful, individualized care.
To truly provide people-centred care, the TB community needs to follow the HIV community in embracing a human-rights framework in the treatment of TB.
Integrating TB into universal health coverage
Last year, at the Global Conference on Primary Health Care in Astana, Kazakhstan, world leaders endorsed a new declaration emphasizing the critical role of primary health care around the world. The declaration states that:
“Strengthening primary health care (PHC) is the most inclusive, effective and efficient approach to enhance people’s physical and mental health, as well as social well-being, and that PHC is a cornerstone of a sustainable health system for universal health coverage (UHC) and health-related Sustainable Development Goals.”
The Lancet Commission argues that progress towards ending TB should occur together with achieving universal health coverage. This means all people have access to high-quality health services — at a minimum, health promotion and primary care — at little or no cost at the point of service.
Given the reality that TB disproportionately affects the poorest, it is critical to ensure that TB services are included within essential universal health-care packages and social protection programs.
It is possible to build a world free of TB. The Lancet Commission report offers countries a road map to achieve these goals and end their TB epidemics. With targeted, proven strategies, smart investments based on sound science, accelerated research and development and a shared responsibility, we can defeat TB within a generation.
Madhukar Pai, Director of Global Health & Professor, McGill University
This article is republished from The Conversation under a Creative Commons license. Read the original article.